Percutaneous Nephrolithotomy (PCNL)
Your consultant has diagnosed that you have a problem with kidney stones and has recommended that you have an operation called a percutaneous nephrolithotomy (nef-roe-lih-THOT-uh-me), or PCNL.
The aim of this procedure is to remove kidney stones by using a ‘keyhole approach’, which is performed by making a small puncture in your back. PCNL has almost completely eliminated the need to use open surgery to remove kidney stones, which is a traditional type of operation where a large incision is made. PCNL also allows patients to recover much faster than patients who undergo open surgery.
This leaflet answers some of the questions you may have about this type of operation. It will help you to understand how the operation is carried out and the care that you can expect to receive afterwards.
If you want to know any more information about the procedure or what the operation involves, please speak to one of the urology doctors or nurses. They will be more than happy to help.
Key points of a PCNL
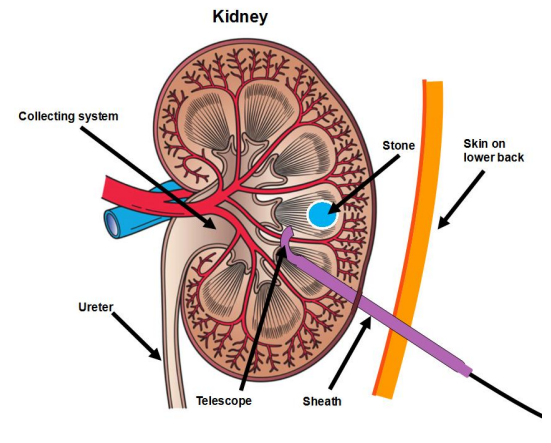
The operation aims to remove all of your kidney stones. It is usually only performed on larger stones, or on patients who have complex kidney anatomy. It is carried out by passing a special instrument into the kidney through a ‘keyhole’ made in the back. The instrument is guided with ultrasound or x-rays and then punctures the kidney, which creates a tunnel to the inside of kidney. A telescope is then passed into the kidney, which is used to find the stones. The stones are then broken up by using a laser, a lithoclast (a small pneumatic drill) or ultrasound.
Details of a PCNL operation
The entire procedure usually takes between one to three hours, depending upon the size of your stone(s).
We normally use a general anaesthetic for this procedure, meaning that you will be asleep throughout the operation. You may be given an antibiotic injection either before or during the procedure. If you are allergic to any antibiotics, please inform staff during your pre-operative assessment, which will be scheduled a few weeks before the operation.
During the procedure a telescopic camera is inserted into your bladder via the urethra (water pipe). The camera is used to insert a small catheter into the ureter (which is a tube that passes urine from the kidney to the bladder) to gain access to your kidney. A catheter is then inserted into your bladder.
After the catheter is successfully inserted, you will be turned over so that your chest faces the operating table. A keyhole incision will be made in your back and an instrument with a special needle will be guided by x-ray or ultrasound in order to puncture the kidney. Once the kidney is punctured, the needle is replaced with a guidewire and devices called dilators are attached to the guidewire in order to form a tunnel into the kidney. A sheath is then inserted into the tunnel, which creates a clear pathway directly into the kidney. A telescope (also called a nephroscope) is then passed through the sheath so it can locate the kidney stone(s).
The stones are broken up using a laser, lithoclast (a small pneumatic drill), or ultrasound. Larger fragments of the stone(s) may be removed with forceps or suction. The laser may also reduce some stones to dust, meaning that the fragments will pass out of the body through the bladder.
A stent will be inserted at the end of the procedure to aid healing. The stent is usually removed in about two to three weeks in the Endoscopy Department. A temporary drainage tube called a nephrostomy tube may also be inserted into your kidney at the end of the procedure. The nephrostomy tube will exit through the skin on your back and will be connected to a urine collection bag. You may get some leakage of urine from the nephrostomy site, but this usually stops within 24 to 48 hours. You will not be discharged until the leakage stops.
It may be necessary to perform a CT scan or an x-ray the day after operation to see if all the stones have been removed.
Will the operation completely cure me?
Although a PCNL should remove all of your kidney stones, it is important to note that more than one operation may be required to clear away all of your stones. You may also form new stones after the operation.
Are there any risks involved in having a PCNL operation?
Most people get through their operation with no problems and are very pleased with the results. However, it is important to realise that complications can sometimes occur. Complications are usually the result of heavy bleeding and/or infection. However, blood in your urine and discomfort are expected side effects following operation.
If you are worried about any of the risks of the operation, please talk to one of the urology doctors or nurses
Getting ready for the operation
A few weeks before the operation, you will be asked to attend a pre-operative assessment, which will check to see if you are medically fit for surgery and/or general anaesthetic. The assessment allows us to carry out blood tests, blood pressure checks, advise on medication, and get a medical history from you. This helps medical staff identify any potential problems in advance and take steps to sort them out beforehand.
During this appointment you will be able to speak to a doctor or nurse about the operation and aftercare, and discuss any worries that you may have.
On the day of the operation
Most people come into hospital on the day of their operation. You will be seen by an anaesthetist and nurses will help you get ready to go into theatre. If you have not already signed a consent form for the operation, one of the urology team will go through this with you.
What sort of anaesthetic will I have?
You will be given a general anaesthetic for this procedure. A general anaesthetic means you will be fully asleep whilst the operation is carried out.
How long will I have to stay in hospital?
This will depend on how quickly you recover following the operation. Most people stay in hospital for between two to five days.
What happens after the operation?
When the operation is over you will have your blood pressure, pulse and breathing checked regularly by the nursing staff. You will have a drip running into a vein in your arm, which will give you fluids until you are able to eat and drink on your own again. There will be a flexible tube (called a catheter) going up the urethra into your bladder, to drain away urine and blood. There may also be tube draining fluid from the kidney called a nephrostomy. This drainage bag will be attached to the catheter and you may find that it looks very bloodstained. This is normal, and will resolve with time.
How long will it take to recover?
The day after the operation you can usually get out of bed and walk around. You should also be able to eat and drink normally. You may feel tired over the next few days, so we advise that you take plenty of rest.
On the morning of your discharge your catheter will be removed. Your urine still may look pink; but this is entirely normal and will clear. We advise you to drink plenty of fluids to help flush the bladder out and improve the colour of the urine.
When the catheter has been removed, you may experience some difficulties, for example needing to pass urine frequently and urgently. You may also experience some dribbling. This is nothing to worry about and is normal. It occurs because it takes time for the bladder and the areas operated on to recover.
Occasionally, it is not possible to pass urine after the operation. If this happens a catheter will need to be placed back into your bladder and will normally stay in for two to four weeks. You will be able to go home with the catheter and the nursing staff on the ward will teach you how to manage and care for the catheter at home. We will then arrange for a district nurse to remove the catheter in the comfort of your own home. Removing a catheter is not normally a painful experience, and once it is removed you should then be able to empty your bladder without difficulty.
What should I do when I get home?
At home you still may see blood in your urine, which is normal and may last for up to four weeks. Just like wounds on your skin, internal wounds from the operation form scabs and eventually drop off, which can cause minor bleeding. If you do notice blood in your urine, please drink plenty of fluids to help flush your system. If the bleeding becomes heavy, or lasts for more than 48 hours, then you should contact your GP for assistance.
After discharge you may continue to pass urine frequently. This should gradually improve over the next few weeks and months. Continue to practice any pelvic floor exercises that you have been taught.
If you experience increasing frequency of needing to pass urine, pain when passing urine, or if you develop a temperature, there is a possibility you may have a urinary tract infection (UTI). If you have any of these symptoms, please contact your GP. Your GP may ask you to provide a urine sample. If a UTI is confirmed you may be asked to take a course of antibiotics.
What exercise can I do?
Strenuous exercise such as gardening, decorating, heavy lifting, golf, and cycling should be avoided for at least two weeks. You should gradually increase your level of activity after that. The speed of recovery will vary from patient to patient, but as a general guide between four to six weeks is seen as normal.
Gentle walking and swimming are beneficial and can be undertaken immediately.
When can I go back to work?
This depends on the type of tasks you do at work. Most ‘light’ jobs may be resumed after four weeks, and any ‘heavy’ jobs should be avoided for at least six weeks.
When can I drive again?
Ultimately it is your responsibility to ensure that you are fit to drive after any surgical procedure. You only need to contact the DVLA if your ability to drive is likely to be affected for more than three months. Checking with your insurance company is the only way to tell when you are legally covered to drive.
What follow up can I expect?
You may be seen in the outpatients department three months after the operation, or you may simply be contacted by telephone.
General things to remember
If you have been given antibiotics after your operation, make sure you complete the entire course. Try not to strain when you go to the toilet. If you become constipated, contact your family doctor (GP) for advice.
Contact numbers
We hope that you have found this information useful. If you have any questions or are worried about anything, please speak to your family doctor (GP) or:
Consultant Urological Surgeons
Mr N Afzal 01305 255468
Mr S Andrews: 01305 255274
Mr A Cornaby: 01305 255470
Mr Z Khan: 01305 255470
Urology Nurse Specialists: 01305 255415
Lulworth Ward: 01305 255471
Abbotsbury Ward: 01305 255481
Continence Advisors: 01305 259978
About this leaflet
Authors: Kirsten Ryan, Urology Nurse Specialist, and Andy Goffe, Urology Nurse Consultant
Editor: Seth Palmer
Written: May 2018
Approved: June 2018
Review date: June 2021
Edition: 1
If you have feedback regarding the accuracy of the information contained in this leaflet, or if you would like a list of references used to develop this leaflet, please email patientinformation.leaflets@dchft.nhs.uk
Print leaflet