Endoscopic Retrograde Cholangio-Pancreatography (ERCP)
What is an ERCP?
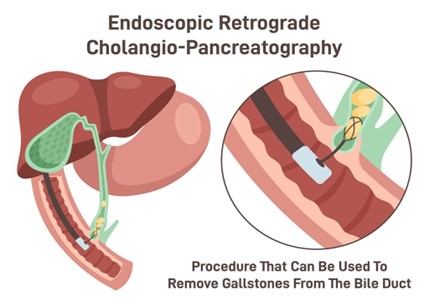
Endoscopic Retrograde Cholangio-Pancreatography (ERCP) is a procedure used to investigate and treat conditions that affect the bile ducts and/or pancreas gland. It is performed using an instrument called an endoscope, which is passed though your mouth into your stomach and small bowel. Dye is passed into the bile and pancreatic ducts, and x-rays are taken to get detailed pictures of any problems. It is performed by a doctor and usually takes 30 to 45 minutes.
Why have an ERCP?
ERCP is usually carried out for investigation and treatment of bile duct stones, blockage of the bile duct causing jaundice or pancreatitis.
What are the benefits of having an ERCP?
During the procedure clear pictures can be obtained of the bile and/or pancreatic ducts allowing an accurate diagnosis of your problem. If there are gallstones ‘stuck’ in the bile duct these can be removed after performing a small internal cut called a sphincterotomy. If there is a blockage/stricture causing jaundice this can be bypassed by inserting a tube called a stent which will help to clear the jaundice. Some stents need to be removed whilst others can be left in permanently.
What are the risks of having an ERCP?
The majority of people who have an ERCP have no serious complications. However, as with all medical procedures, there are some side-effects and risks. It is not uncommon to have a sore throat after the procedure. Some people experience some abdominal discomfort afterwards, because of the gas that has been put into the stomach. This usually settles by itself within a few hours. There are some risks, which we need to make you aware of:
- Sedation / anaesthesia: There is a slight risk of developing a chest infection following an ERCP. Because of sedation / anaesthetic there is a small chance of heart and lung problems during or after the procedure. These complications are rare but potentially very serious and even life-threatening (i.e. including a very small, but not zero, risk of death). The risk of complications is higher if you are overweight or if you already have heart or lung problems or are in poor general health. Your doctors will have carefully weighed up the benefit of this procedure against the risk of complications.
- Pancreatitis: Inflammation of the pancreas sometimes occurs after an ERCP. The risk of pancreatitis from having an ERCP varies from person to person and typically occurs in four in 100 cases. If you develop pancreatitis you will experience abdominal pain and will need to stay in hospital. There is no effective treatment for pancreatitis and it is usual to need an intravenous drip and pain killers. Rarely it is more serious and can require a longer stay in hospital or an operation and may even be life-threatening (i.e. again, including a very small but not zero risk of death). The risk of developing pancreatitis can be significantly reduced using an anti-inflammatory drug called diclofenac (also known as Voltarol). This is administered as a suppository (into the back passage) whilst you are still under sedation.
- Bleeding: If a cut is made into the opening of the bile duct (sphincterotomy) there is a risk of bleeding in one in 100 cases. This usually settles by itself. Rarely, a blood transfusion, further endoscopy or even an operation may be required.
- Perforation: Rarely, a small tear (perforation) may be made in the gut lining. The risk of perforation during ERCP is one in 200 cases. It can be treated by resting the gut and giving intravenous fluids. Surgery may be required.
- Infection: Infection of the bile duct (cholangitis) may occur after an ERCP in two in 100 cases. This requires treatment with antibiotics if it occurs.
- Incomplete procedure: There is about a one in 10 chance that the procedure may only be partially successful. If this is the case, your doctors will discuss further treatment options with you. It may be necessary to repeat the procedure.
If you experience any complications after your procedure, please seek urgent advice. Contact details will be given at discharge.
Is there an alternative to ERCP?
Yes, but this has been recommended for you because it is an effective way of investigating your and judged to be safer than the alternatives, such as open surgery. This is a voluntary investigation and if you are unsure, please seek more information from your referring doctor or from the Endoscopy Department.
How do I prepare for an ERCP?
- Do not have anything to eat or drink for at least six hours before the procedure
- Take all of your usual medication on the morning of the procedure. If you have diabetes, or take any of the medications listed above, then please call the Endoscopy Unit to receive instruction on which medications need to be stopped
- Bring ALL of your medications with you
- Arrange for someone to collect and accompany you for at least 24 hours after the procedure (you will not be able to drive or work for 24 hours afterwards)
- Pack and bring an overnight bag in case you are required to stay in hospital after the procedure. Please also bring a dressing gown and slippers for your comfort and dignity
- Please read the entire booklet. You will have an opportunity to ask any further questions and to sign a consent form with a health professional on the day.
Planning your care
If you are taking any of the following medications, or have any of the medical conditions listed below, please contact the Clinical Advice Line on 01305 253152 to help us plan appropriate care and management of your condition during your visit with us.
| Do the following apply? | If yes: |
| Do you have a long-term condition such as epilepsy, Parkinson’s, chronic pain and steroid deficiency e.g., Addison’s (adrenal deficiency)? | Call Clinical Advice Line |
| Diabetes | Call appointments to ensure appropriate appointment; see diabetic leaflet |
| Recent heart attack Cardiac pacemaker or ICD fitted | Call Clinical Advice Line |
| Aspirin OR Dipyridamole therapy | Continue as normal |
| Warfarin therapy | You will receive written instructions on when to stop these medications |
| Clopidogrel, Ticagrelor, Prasugrel therapy | |
| Dabigatran, Rivaroxaban, Apixaban, Edoxaban therapy | |
| Anti-hypertensives to lower your blood pressure | Call Clinical Advice Line |
| Diuretics (water tablets) | |
| NSAID’s (non-steroidal anti-inflammatory drugs), such as Ibuprofen or Meloxicam | |
| Or if you have ever had an allergic reaction to ‘contrast’ used in an X-ray examination | Call Clinical Advice Line |
On the day of the procedure
Patients will need to make arrangements to be taken home after the procedure and under no circumstances should undertake this journey alone.
What happens when I get to the Endoscopy Department?
When you come to the Endoscopy Unit, please give your name to the receptionist. A nurse will come to meet you and take you through to a private office. You will be asked some questions about the arrangements you have made to get home and about your health. Please tell the nurse if you are allergic to any medicines. You can ask any questions that you have or tell the nurse of any worries.
The nurse will take your pulse and blood pressure and ask you to get changed into a hospital gown ready for the test.
Please note that x-rays will be taken during the test and if you could be pregnant please inform the staff.
Signing the consent form
You will have been sent a consent form as part of your admissions pack, please read this before your procedure. You will have a chance to speak to your endoscopist before the procedure to discuss any concerns, and to sign the consent form. Please bring this form with you on the day.
The endoscopist will come and meet you to discuss the procedure. It is important before signing that you understand what is likely to happen and that you have asked any questions that you feel necessary to make up your mind. Please read the advice on consent that is in this booklet.
Who will be in the procedure room with me?
You will be accompanied into the procedure room by a nurse or doctor. Also present will be more nurses, an anaesthetic doctor and their assistants. Nursing students and medical staff in training may be present in the room to observe the procedure. The ERCP procedure will be performed by a consultant gastroenterologist or surgeon.
The ERCP examination
There are many people involved in providing safe ERCP. After you enter the room, the nurses will go through a final checklist with you. You will be asked to lie on your back on a trolley so that a small needle can be placed in your hand or arm to allow us to give you medication for the procedure. Most ERCP procedures are conducted using heavy sedation given by an anaesthetist. Alternatively, you may be given a combination of a sedative to make you sleepy, a painkiller to keep you comfortable, and a muscle relaxant to help control the movement of the gut. These do not make you unconscious, although many patients are very sleepy within a few minutes. You may have some awareness during the procedure however most people do not remember anything and are comfortable throughout.
You will be asked to remove any false teeth, spectacles or contact lenses. Your pulse, blood pressure, breathing rate, oxygen levels and heart rhythm will be monitored throughout the procedure. To do this we will place a soft clip on your finger, a cuff around your upper arm, and stickers on your back. We will also give you oxygen via a mask. You will then be asked to turn over onto your front. A mouth guard will be placed between your teeth and gums to protect them and to prevent damage to the endoscope.
The doctor will pass the endoscope through your mouth, down into your stomach and then into your small bowel (duodenum). A fine tube is then passed down the endoscope and inserted into your bile duct. Dye is injected through this tube and x-rays are taken. The dye passes out of your body harmlessly.
If the x-ray shows a gallstone stuck in the bile duct the doctor will undertake a sphincterotomy which is a procedure to enlarge the opening of the bile duct by cutting through the ring of muscle fibres that forms a tight nozzle at the bottom of the bile duct. This is performed using a heated wire (diathermy), which you will not feel. The stones can then be removed using specially design instruments and then allowed to pass naturally in your bowel motions.
Occasionally, it may not be possible to remove the stone/s from the duct and you may have to come back after an interval for a further attempt. If this is the case, a small plastic tube called a stent may be placed so that it bypasses the stone/s and allows bile to flow freely from the liver into the duodenum.
If a narrowing or blockage is found, the doctor can insert a plastic or wire mesh stent inside to open it wider and allow the bile to flow. You will not be able to feel the stent inside you. Depending on the type of stent used, further endoscopic procedures may be necessary to remove, replace, service, or unblock it.
Occasionally, small samples may be taken from the bile duct or near the opening of it. Photographs of your small intestine may also be taken and stored as part of your medical records.
After the procedure
You will be transferred to the Recovery Area where you will be monitored closely until you are fully awake. You will be kept nil by mouth until you have fully recovered from the sedation. If all is well, you will normally be allowed to drink clear fluids after 2 hours and start eating a light diet after a further 2 hours if no problems arise. The endoscopist may alter these directions depending on the outcome of your ERCP.
Going home
You are likely to be allowed home the same day.
Please arrange to have a relative or friend available to collect you from inside the unit, drive you home and look after you for 24 hours. Please bring these contact details with you and give them to the nursing team.
A member of staff will discuss the results of the ERCP with you and provide you and your escort with discharge information.
For 24 hours after the procedure you should not:
- Have an alcoholic drink
- Drive a car
- Operate machinery
- Sign legally binding documents
- Be responsible for young children
If the Endoscopist decides you need to stay in hospital overnight for observation, a bed will be made available on one of our wards. They will explain any further investigations or follow up that you may need.
If you experience any problems related to your visit to Endoscopy, including the need to see your GP or attend hospital, please let the department know. A brief written summary would be helpful. We welcome all feedback to enable us to further improve the service offered.
If you feel unwell after discharge
If any of the following occur within 48 hours after having the ERCP, you must contact a doctor or attend the Emergency Department immediately:
- Severe pain in your abdomen (tummy)
- Fever (raised temperature)
- Difficulty breathing
- Vomiting blood or passing black motions
Taking a copy of your discharge advice can help to ensure that you receive prompt investigation and treatment.
Please note: individuals are unable to donate blood for four to six months after flexible endoscopy and until they have informed the blood service of the diagnosis.
We are privileged to be a training hospital
There may be a trainee Endoscopist observing or performing your procedure. If this is the case, there will also be a fully trained accredited Endoscopist present. You will be informed during your admission. You do have the right to decline their participation in your procedure; please let the admitting nurse know of your wishes.
Your appointment time is the time you are expected to arrive in the department. However, you should plan to be in the Endoscopy Unit for three to four hours. The department has three procedure rooms running at the same time also accommodates emergencies. Someone with a later appointment time may be seen before you. If you have any concerns, please ask a member of staff.
Getting here
Car parking across the main hospital site – including the multi-storey car park – operates using automatic number plate recognition.
As you enter our site via Williams Avenue or Damers Road you will need to take a ticket at the barrier to be able to pass through. This also applies if you are dropping off/picking up or a Blue Badge holder.
When you enter the hospital grounds, follow the signs for North Wing Entrance 1. The Endoscopy Unit will be signposted as you enter the main entrance.
Contact numbers
Endoscopy Unit main reception: 01305 255225
Appointment enquiries: 01305 255701
Clinical Advice Line (medical enquiries): 01305 253152
If you call the Clinical Advice Line and your call goes to answer phone, please leave a message with the following details:
- Your name and telephone number
- The procedure you are having
- Date and time of your appointment
- Your reference number (hospital number) or our reference number (NHS number)
- Your query.
Someone will return your call as soon as possible to discuss your telephone message with you.
If you are using hospital transport and your appointment is after 2pm, please contact the appointments line to rearrange an earlier appointment.
Patients’ property
You are advised not to bring expensive items of jewellery or clothing with you when you visit the Endoscopy Unit.
You will be given a patient property bag to place your clothes in.
You will be asked to keep your property with you at all times.
The Endoscopy Unit and Dorset County Hospital NHS Foundation Trust cannot accept responsibility for the safeguarding your property.
About this leaflet
Author: Dr James Jupp, Consultant Gastroenterologist
Written: May 2018
Reviewed: January 2026
Reviewed by: Dinsdale Marjoram and Mr Kyle Mitchell Consultant Surgeon
Review date: December 2028
Edition: v3